

What Do I Do If I Have Liver Disease?
A practical, step-by-step plan: confirm what you have, reduce the driver, monitor what matters, and know when care is urgent. [1] [2]
Overview
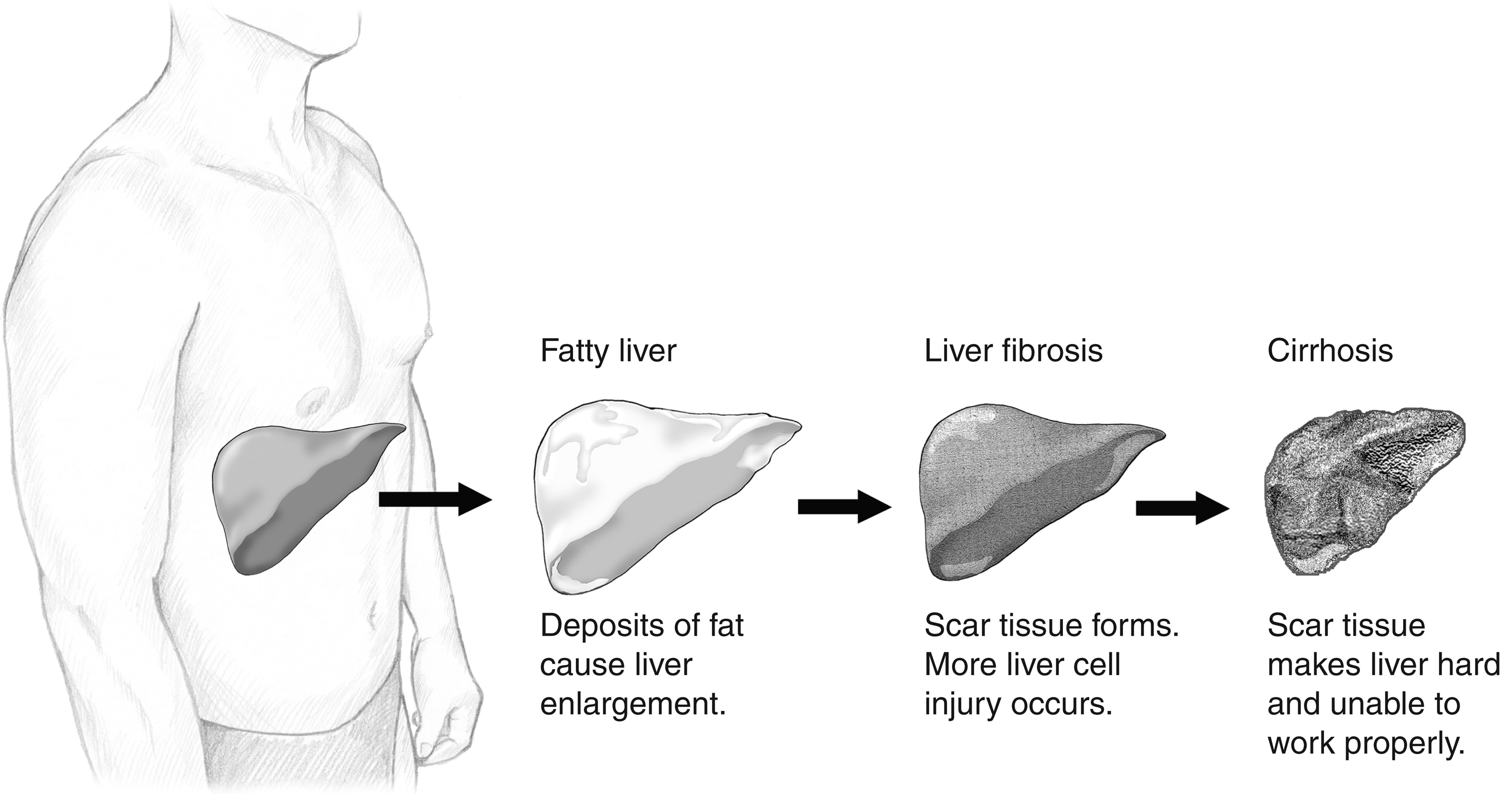
“Liver disease” is an umbrella term—it can mean mild inflammation, fatty liver, significant fibrosis, or cirrhosis. The right next step depends on cause (alcohol, metabolic/MASLD, viral hepatitis, autoimmune, medication-related, etc.) and stage (no scarring vs advanced scarring). [1] [3]
The goal is not to “Google your way to certainty.” The goal is to take organized action: confirm the diagnosis, stop the driver, prevent complications, and make sure you know what symptoms are emergencies. [2]
First 48 Hours: Get Oriented
- Confirm what “liver disease” means in your case. Ask: “Do I have fatty liver, fibrosis, cirrhosis, hepatitis, or something else?” [1]
- Clarify cause (etiology). The cause drives treatment: alcohol-associated liver disease, MASLD/MASH, hepatitis B/C, autoimmune hepatitis, medication/toxin, hereditary conditions, and more. [3] [7]
- Clarify stage (especially whether cirrhosis is present). Cirrhosis means permanent scarring and higher risk of complications; many people don’t feel symptoms until late. [2]
- Ask whether a hepatology referral is appropriate. Referral is especially important if there are complications, suspected decompensation, or need for endoscopy/HCC surveillance. [5]
Stabilize the Basics (What You Can Control)
Most liver diseases improve when the driver is removed or controlled—sometimes dramatically. Your clinician should guide the plan, but these are common pillars: [1]
- If alcohol is the driver: stopping alcohol is foundational (and often urgent). Ask about safe withdrawal planning if you drink heavily. [7]
- If MASLD/MASH is the driver: metabolic management (weight, diabetes, lipids, BP) matters because it changes progression risk. [8]
- If viral hepatitis is the driver: treatment and monitoring can change long-term outcomes and reduce complications. [9] [10]
- If autoimmune hepatitis is the driver: controlling immune-mediated inflammation reduces progression risk (requires specialist oversight). [11]
- Medication safety: do not start supplements or “liver cleanses” without your team; review all meds (including OTC and herbals). [1]
Monitoring and Follow-Up (What Teams Track)
Monitoring depends on stage. In earlier disease, the focus is on cause control and fibrosis risk. In cirrhosis, the focus expands to complications, surveillance, and transplant planning when appropriate. [2] [5]
- Labs and trends: liver enzymes (AST/ALT), bilirubin, INR, albumin, platelets, and kidney function are commonly used to assess severity and trajectory. [2]
- Fibrosis assessment: elastography and/or other noninvasive tests may be used to estimate scarring and monitor change over time. [1]
- If cirrhosis: outpatient management includes preventing/monitoring complications (ascites, encephalopathy, variceal bleeding) and ensuring appropriate surveillance/referral. [5]
- Ascites is a major inflection point: clinically significant ascites and related complications should prompt consideration of transplant evaluation (when appropriate). [13]
When It’s Urgent (Do Not Wait)
Liver disease can worsen quickly, especially when bleeding, infection, dehydration, kidney injury, or encephalopathy enter the picture. If any of the following occur, seek urgent/emergency care based on your team’s instructions and local emergency services. [6]
- Vomiting blood or black/tarry stools (possible GI bleeding). [6]
- Severe confusion, extreme sleepiness, or inability to stay awake/answer normally (possible encephalopathy). [6]
- Fever with abdominal pain/tenderness or rapidly worsening swelling (possible infection such as SBP—especially in cirrhosis). [13]
- New or rapidly worsening jaundice, severe abdominal pain, fainting, or shortness of breath. [14] [15]
Questions to Ask Your Clinician or Transplant Team
- What is the most likely cause of my liver disease, and what is the plan to treat that cause? [3]
- What is my current stage (fatty liver, fibrosis, cirrhosis), and what test supports that conclusion? [2]
- Do I have any signs of decompensation (ascites, bleeding risk, encephalopathy), and what should I do if symptoms appear? [5] [6]
- How often should I have labs/imaging, and which results matter most to you (trend vs single value)? [1]
- Should I be referred to hepatology—and if cirrhosis or significant ascites is present, is transplant evaluation appropriate to discuss now? [5] [13]
References
- AASLD. Practice Guidelines (evidence-based guidance for clinicians; useful starting point for what “standard evaluation/management” means).
- NIDDK/NIH. Cirrhosis: Definition & Facts (overview; notes many people have no symptoms until late).
- NCBI Bookshelf (NIH) — StatPearls. Hepatic Cirrhosis (overview of causes and progression framework).
- NIDDK/NIH Media Asset. Normal Liver, Fatty Liver, Liver Fibrosis, and Cirrhosis (image; please credit NIDDK/NIH).
- AASLD Liver Fellow Network. Back to Basics: Outpatient Management of Cirrhosis (referral considerations; ambulatory management framework).
- U.S. Department of Veterans Affairs (VA). Cirrhosis: When to go to the emergency room (patient guidance on bleeding/confusion red flags).
- Crabb DW, Im GY, Szabo G, et al. (PubMed). Diagnosis and treatment of alcohol-associated liver diseases (AASLD guidance framework).
- Rinella ME, Lazarus JV, Ratziu V, et al. (PubMed). Consensus/guidance on NAFLD/MASLD (metabolic drivers and management direction).
- CDC. Hepatitis C: Signs and symptoms (patient-facing symptom guidance).
- CDC. Hepatitis B: Symptoms (patient-facing symptom guidance).
- Manns MP, Lohse AW, Vergani D. (PubMed). Autoimmune hepatitis (diagnosis/management principles and outcomes overview).
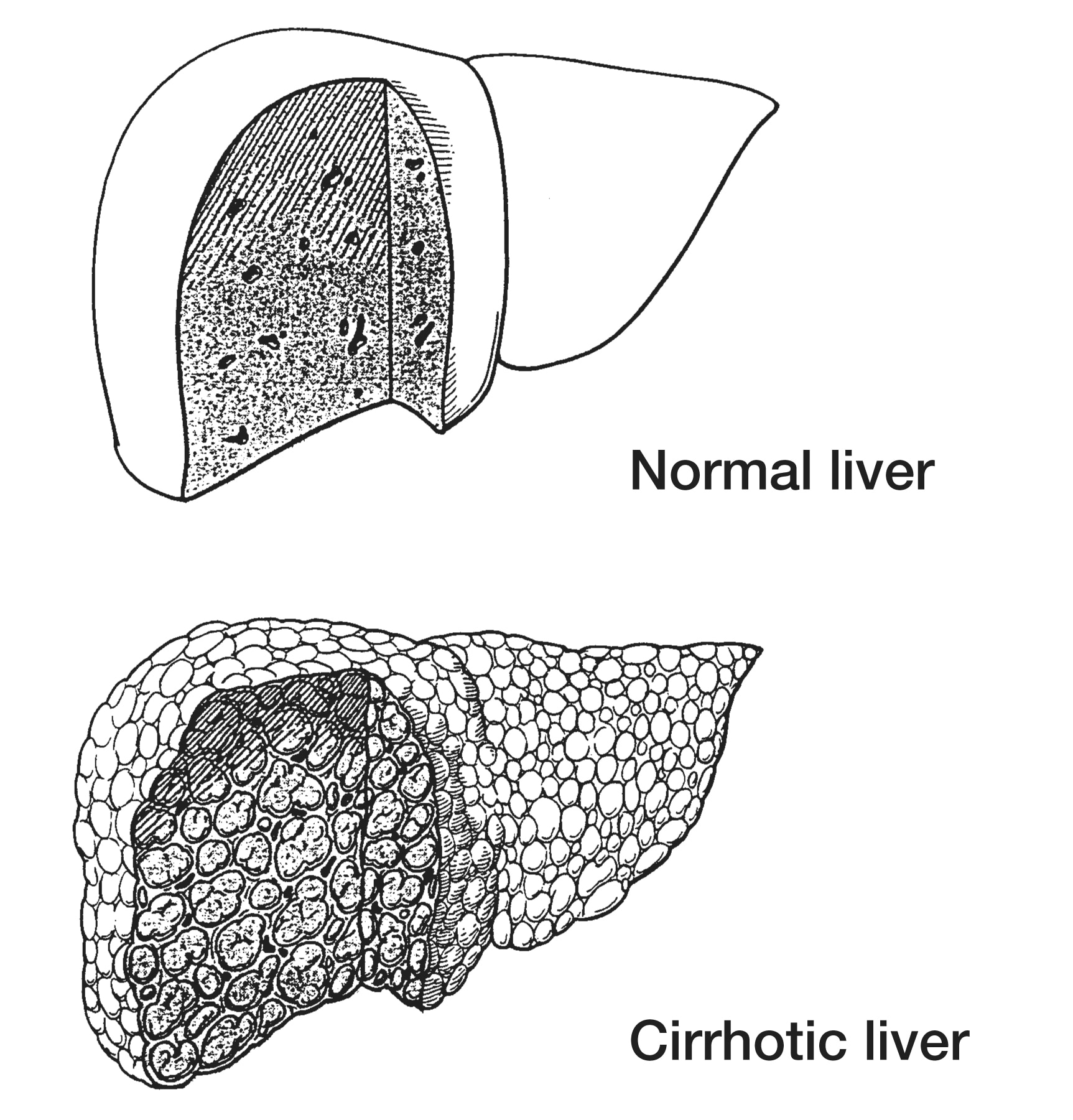
- NIDDK/NIH Media Asset. Portions of normal and cirrhotic liver tissues (image; please credit NIDDK/NIH).
- AASLD. Diagnosis, Evaluation and Management of Ascites, SBP, and HRS (notes transplant evaluation considerations in clinically significant ascites).
- NIDDK/NIH. Cirrhosis (patient overview and complications context).
- CDC. Clinical Signs and Symptoms of Hepatitis B (clinical-oriented list including jaundice/dark urine/clay stools).