
Do I Have Liver Disease?
A calm, practical way to think through symptoms, labs, and risk factors—before panic or denial takes over. [2]
Overview
This is usually how it starts: a “mildly elevated liver test,” a strange fatigue you can’t explain, a comment on an ultrasound, or a family member who looks at you and says, “Maybe you should get checked.” The problem is that liver disease rarely announces itself cleanly. Many people feel normal for years because the liver has significant physiologic reserve. That resilience is helpful—until it isn’t. The practical way forward is a structured approach: confirm abnormalities, classify the lab pattern, and then evaluate likely causes based on risk. [2]
The goal of this post is not to diagnose you. It is to help you think clearly and talk effectively with your clinician. If you’re early in the process, you need a plan that prevents two extremes: panic (“This must be cirrhosis”) and dismissal (“It’s probably nothing”). Many causes of liver injury are treatable—especially when identified early—and a stepwise evaluation is designed to find what matters without wasted testing. [3]
Common Signs (and Why They Can Mislead)
Symptoms are a noisy signal. Fatigue, low appetite, mild nausea, or “brain fog” can occur in liver disease, but they also occur with sleep disruption, medication effects, thyroid disease, anemia, depression, and many other conditions. This is why clinicians rely heavily on objective patterns—labs, trends, imaging, and risk profile—rather than symptoms alone. A structured approach is specifically recommended for abnormal liver chemistries because it improves diagnostic accuracy and reduces unnecessary testing. [2]
- Fatigue or low energy — common and nonspecific; important mainly when paired with abnormal labs or clear risk factors. [3]
- Abnormal AST/ALT — the degree of elevation does not reliably reflect fibrosis stage; persistence and pattern are more informative. [1] [2]
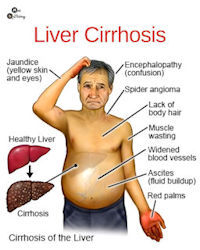
- Red flags (jaundice, confusion, vomiting blood, black stools, significant abdominal swelling) — can signal decompensation and require urgent evaluation. [6]
Labs & Patterns: “Enzymes” vs “Function”
A common misunderstanding is that “liver tests” always measure how well the liver works. Many common labs are markers of injury or bile flow. AST and ALT typically rise with hepatocellular injury; alkaline phosphatase is often higher with cholestatic/bile-duct patterns; bilirubin reflects processing and excretion. “Function” is more directly reflected by labs such as INR and albumin (and, clinically, platelet trends can suggest evolving portal hypertension over time). The recommended first step is to define the pattern (hepatocellular vs cholestatic vs mixed), confirm persistence, and then test likely causes based on history. [2]
This distinction matters because mild AST/ALT elevations can be transient (intercurrent illness, exercise, medications), while rising bilirubin/INR—especially with symptoms—can reflect limited reserve. A stepwise, pattern-based evaluation helps avoid both undertreatment and overtesting. [1] [2]
Risk Factors That Warrant Evaluation
Liver disease usually has a driver. The most common drivers include metabolic liver disease (MASLD/MASH), alcohol-associated liver disease, chronic viral hepatitis, medication/supplement injury, autoimmune disease, and hereditary disorders. Guidance recommends risk-factor review early because it meaningfully improves diagnostic yield and helps clinicians choose targeted testing rather than broad panels without a plan. [2]
- Metabolic risk (diabetes, obesity, metabolic syndrome) — associated with MASLD/MASH and fibrosis risk. [7]
- Alcohol exposure (heavy/prolonged use) — abstinence can materially change trajectory; ongoing intake increases risk. [8]
- Viral hepatitis exposure (HBV/HCV risk) — screening and treatment reduce progression. [9]
- Persistent abnormalities, autoimmune history, or family history — warrants a deliberate workup. [1]
What to Do Next
The most effective next step is usually a structured visit with your clinician (primary care, gastroenterology, or hepatology). In general: confirm abnormal tests, define the pattern, and then test the most likely causes based on your risks and history. If abnormalities persist or risks are meaningful, ask whether fibrosis assessment is appropriate; modern noninvasive tests can help clarify risk and guide surveillance. [2] [10]
- Today: gather your last 6–12 months of labs and imaging; list medications and supplements. [2]
- This month: confirm persistence; ask for a stepwise plan; consider fibrosis assessment when appropriate. [10]
- Emergency: go now for vomiting blood, black stools, severe confusion, fainting, severe shortness of breath, fever with worsening abdominal pain, or rapidly worsening jaundice. [6]
Questions to Ask Your Clinician
- Which pattern do my labs fit (hepatocellular, cholestatic, mixed), and what are the top causes in my case? [2]
- Should we repeat the panel, and if it stays abnormal, what is the stepwise plan? [2]
- Do I need fibrosis assessment now, and how will it change surveillance or management? [10]
- What red flags should trigger urgent care in my situation? [6]
References
- AASLD Liver Fellow Network. How to approach elevated liver enzymes? (Back to Basics).
- Kwo PY, Cohen SM, Lim JK. (American Journal of Gastroenterology, 2017). ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries.
- NIDDK/NIH. Liver disease overview (patient education).
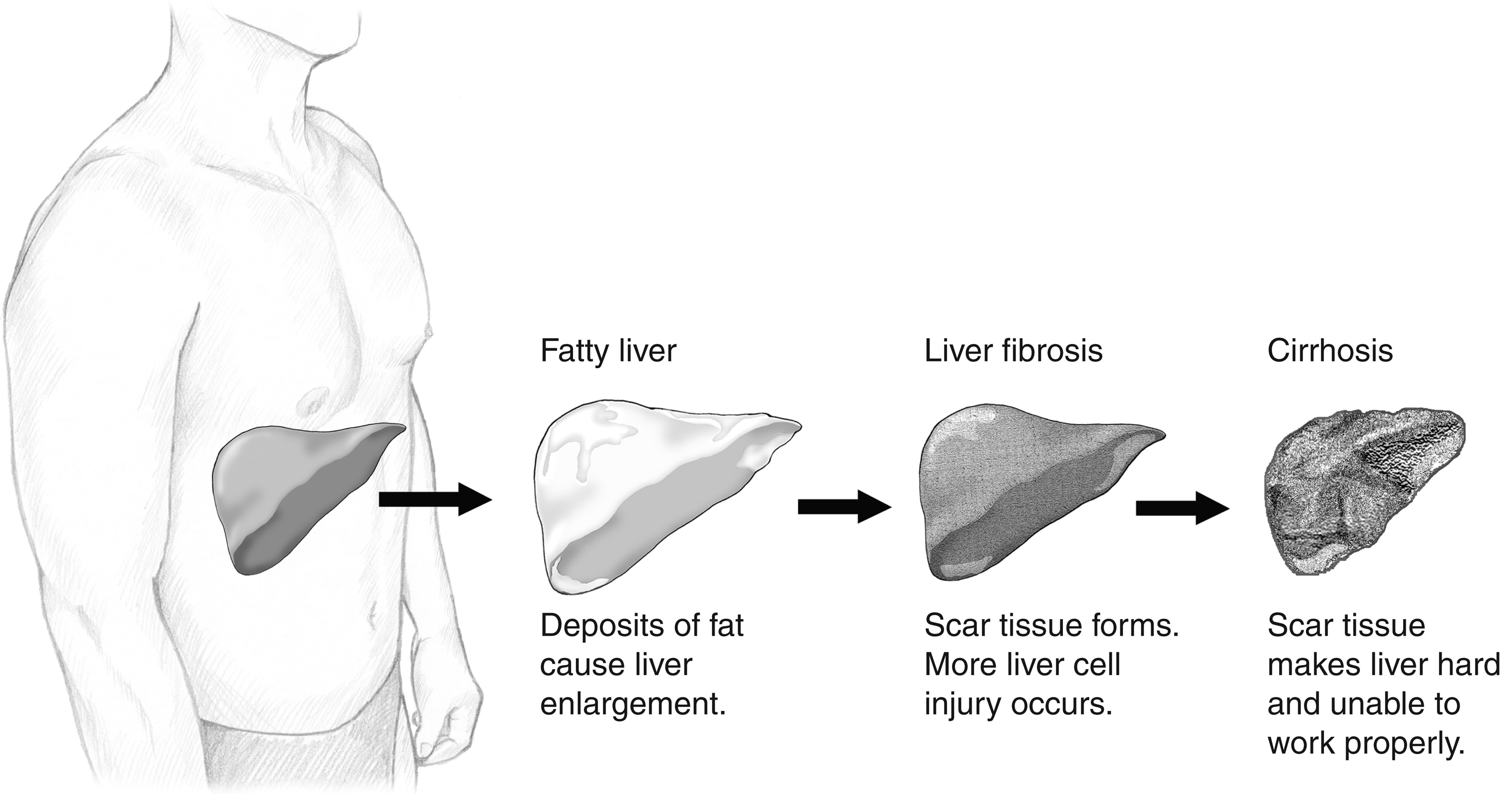
- NIDDK/NIH Media Asset. Normal liver, fatty liver, liver fibrosis, and cirrhosis (image).
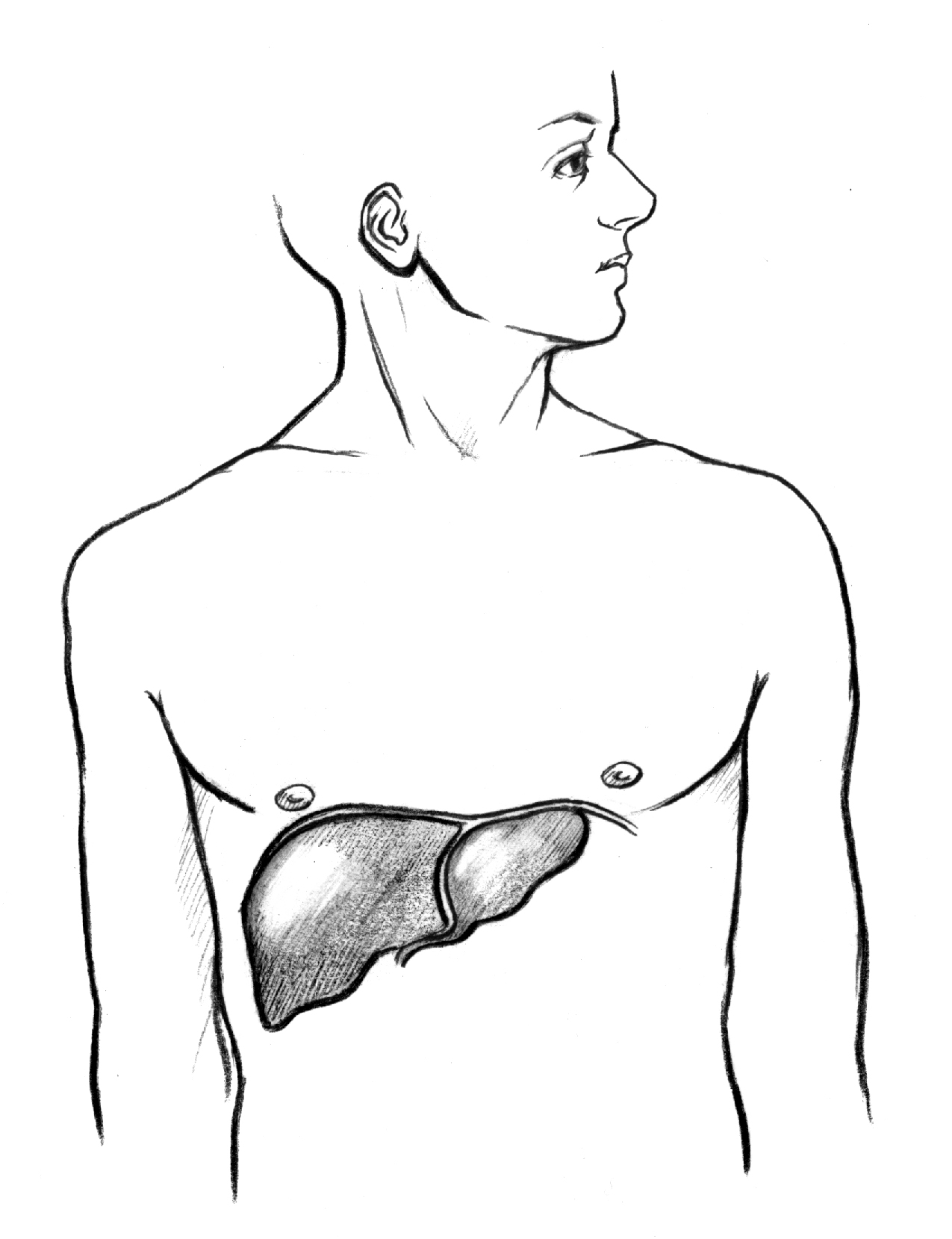
- NIDDK/NIH Media Asset. The location of the liver within the human body (image).
- D’Amico G, Garcia-Tsao G, Pagliaro L. (PubMed). Natural history and prognostic indicators of survival in cirrhosis: systematic review.
- NIDDK/NIH. NAFLD/MASLD overview (patient education).
- Crabb DW, Im GY, Szabo G, et al. (PubMed). Diagnosis and treatment of alcohol-associated liver diseases.
- Terrault NA, Lok ASF, McMahon BJ, et al. (PubMed). Update on prevention, diagnosis, and treatment of chronic hepatitis B.
- AASLD Liver Fellow Network. Back to Basics: Non-invasive Testing for Liver Fibrosis.