
Thrombocytopenia & Liver Disease
Why platelets fall in cirrhosis, what the numbers really mean for bleeding and procedures, and how low platelets affect transplant planning.
Overview
Thrombocytopenia means a low platelet count. In chronic liver disease (especially cirrhosis), low platelets are common and often reflect portal hypertension and splenic sequestration (“hypersplenism”), along with reduced hepatic production of thrombopoietin (TPO) and other contributing factors [1].
A key point for patients: low platelets do not automatically mean you will bleed. In cirrhosis, bleeding risk depends on the whole clinical picture—portal hypertension, varices, infection, kidney function, medications, and what procedure (if any) is planned—rather than one lab value alone [2].
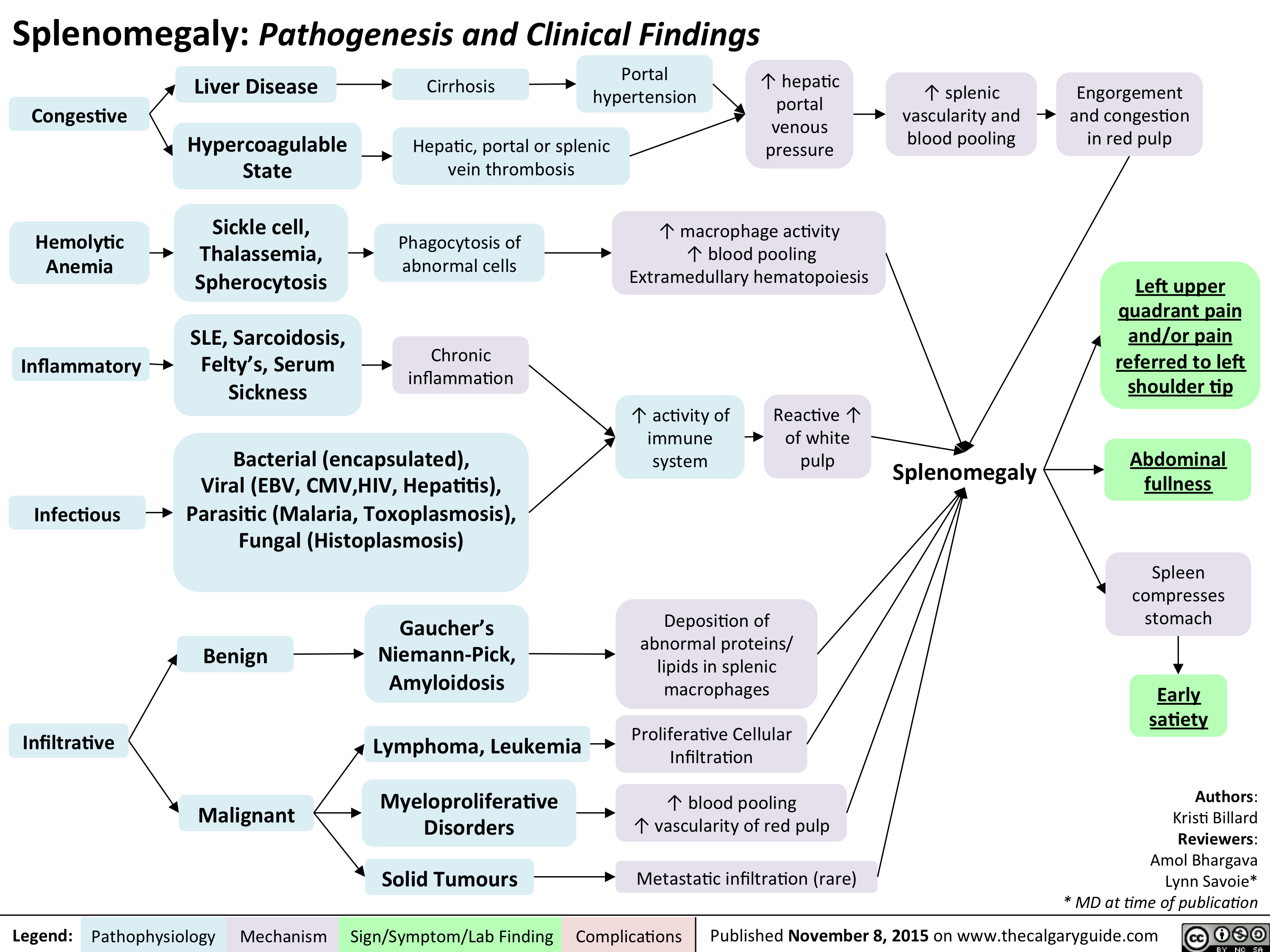
Splenomegaly and “pooling” can contribute to low platelets in portal hypertension. (Educational diagram.)
Why Platelets Drop in Liver Disease
In cirrhosis, thrombocytopenia is usually multifactorial:
- Splenic sequestration (hypersplenism): portal hypertension enlarges the spleen and increases trapping/pooling of platelets [1].
- Reduced TPO production: the liver produces thrombopoietin, a key hormone for platelet production; advanced liver dysfunction can lower TPO [3].
- Bone marrow suppression: alcohol, viral infections, medications, and inflammation can reduce platelet production [1].
- Immune-mediated platelet destruction: some patients have overlapping immune mechanisms that increase platelet clearance [1].
Clinically, a falling platelet count can also function as a clue to portal hypertension severity in the right context, and it is used in some non-invasive risk tools alongside elastography/liver stiffness [4].
How It’s Evaluated
In a patient with known cirrhosis and splenomegaly, mild-to-moderate thrombocytopenia is often expected. Even so, your team should still consider other contributors—because the management differs.
- Trend matters: a slow stable count is different from a rapid drop.
- Medication review: antibiotics, antivirals, heparin exposure, chemotherapy, and other drugs can affect platelets.
- Alcohol and viral activity: ongoing alcohol use or active viral hepatitis can worsen marrow suppression.
- Blood smear / labs as needed: to check for clumping, hemolysis, or other hematologic patterns.
For procedure planning, many centers focus less on “why” in the moment and more on what the safest hemostasis strategy is for this specific procedure [5].
Bleeding Risk vs the Platelet Number
In cirrhosis, the clotting system is often described as “rebalanced”—meaning both bleeding and clotting risks can coexist. Platelet count is only one component of that balance [5].
Practical takeaways:
- Mild thrombocytopenia is common and often does not require treatment by itself.
- Severe thrombocytopenia (often discussed around <50,000/µL for higher-risk procedures) can complicate invasive care and may need a targeted strategy [6].
- If you have varices, the bleeding risk story is dominated by portal hypertension and variceal management—not just platelet count.
Procedures & Platelet Thresholds
For cirrhosis patients, different societies and centers use different thresholds depending on the procedure type and patient context. Many contemporary approaches emphasize individualized decision-making rather than a universal cutoff [2].
Examples of commonly cited targets for higher bleeding-risk procedures:
- Some interventional radiology guidance uses ~30 × 109/L as a threshold in selected settings [2].
- GI societies (AGA/ACG) are often cited around ~50 × 109/L for higher-risk procedures [2].
The most important operational point: follow your transplant/hepatology team’s plan for your specific procedure (paracentesis, endoscopy, liver biopsy, dental work, surgery), because risk varies enormously by procedure and by your current clinical status [5].
Treatment Options
Treatment is guided by why the platelets are low and what you need to do safely (especially if a procedure is planned).
1) Treat the liver disease and portal hypertension drivers
- Address alcohol use disorder, viral hepatitis activity, nutrition, and infections when present.
- Manage portal-hypertension complications using guideline-based strategies (varices, ascites, etc.).
2) Platelet transfusion (situational)
Platelet transfusions may be used around urgent or high-risk procedures, but effects can be short-lived in hypersplenism and portal hypertension, and transfusion strategies vary by center [6].
3) TPO receptor agonists for planned procedures (selected patients)
Two oral medications—avatrombopag and lusutrombopag—have randomized trial evidence showing reduced need for platelet transfusion or “rescue” bleeding procedures in chronic liver disease patients with thrombocytopenia undergoing scheduled invasive procedures [7] [8].
- These are typically used short-term before a scheduled procedure, not as indefinite “platelet boosters.”
- They must be coordinated with your transplant/hepatology team, who will weigh benefits vs risks (including thrombotic risk in selected patients).
The best plan is the one that matches your current stability, the procedure type, and your transplant center’s protocols [2].
Transplant Implications
In advanced cirrhosis, thrombocytopenia often reflects clinically significant portal hypertension and splenic sequestration [1]. For many patients, low platelets are part of the “decompensation ecosystem” that also includes varices, ascites, and encephalopathy.
Practical transplant-relevant points:
- Pre-transplant: low platelets may complicate biopsies, dental work, endoscopies, or surgeries; planning and coordination matter more than panic.
- At transplant admission: your surgical/anesthesia team will manage coagulation dynamically (labs, transfusion strategies, and hemostasis).
- Post-transplant: platelet counts often improve as portal hypertension resolves, but early post-op thrombocytopenia can also occur for other reasons (consumption, infection, medications), so monitoring continues.
If your platelet count is falling quickly, or if it is out of proportion to other liver findings, your team may broaden the workup beyond “hypersplenism” [5].
When to Seek Urgent Care
Seek urgent evaluation (or emergency care) for:
- Vomiting blood, black/tarry stools, or passing large amounts of blood (possible GI bleed).
- New severe headache, weakness, fainting, or confusion.
- Bleeding that will not stop, large spontaneous bruises, or bleeding plus fever.
- Any sudden, concerning change after a procedure.
Remember: in cirrhosis, major bleeding events are often driven by portal-hypertension complications (like varices) and acute illness triggers, so fast evaluation is critical [4].
Questions to Ask Your Liver or Transplant Team
- What do you think is the main cause of my low platelets—splenic sequestration, low TPO, medications, or something else? [1]
- For my next procedure, what platelet threshold (if any) are we targeting, and why? [2]
- Should we consider a TPO-receptor agonist (avatrombopag or lusutrombopag) instead of transfusion for a planned procedure? [7] [8]
- Are there medications or supplements I should avoid because they increase bleeding risk or affect platelets?
- What symptoms should trigger an immediate call to the team or a trip to the emergency department?
References
- Peck-Radosavljevic M. Thrombocytopenia in chronic liver disease. Liver International. 2017.
- AASLD Liver Fellow Network. Peri-procedural management of bleeding risk in cirrhosis. (Updated resource.)
- Poordad F. Review article: thrombocytopenia in chronic liver disease. Aliment Pharmacol Ther. 2007.
- de Franchis R, et al. Baveno VII – Renewing consensus in portal hypertension. J Hepatol. 2022.
- Fortea JI, et al. Periprocedural management of hemostatic alterations in patients with cirrhosis. 2023. (Open access, PMC)
- Biolato M, et al. Minimum platelet count threshold before invasive procedures in cirrhosis: evolution of the guidelines. 2023. (Open access, PMC)
- Terrault N, et al. Avatrombopag before procedures reduces need for platelet transfusion in chronic liver disease with thrombocytopenia (phase 3 trials). 2018.
- Peck-Radosavljevic M, et al. Lusutrombopag for thrombocytopenia in chronic liver disease undergoing invasive procedures (L-PLUS 2). 2019.