
Stages of Liver Disease
A pure-story walkthrough of how four common pathways can move from quiet injury to decompensation—and why MELD and Child–Pugh matter along the way.
Overview
Imagine four patients starting on the same calendar date: one drinking heavily, one living with metabolic dysfunction–associated steatotic liver disease (MASLD) and steatohepatitis (MASH), one carrying chronic viral hepatitis, and one with autoimmune hepatitis smoldering in the background. They do not share the same pace, but they share a recognizable arc: repeated injury, scar formation, architectural distortion, and then a tipping point where the liver can no longer compensate. Clinicians map this journey using fibrosis stage, the presence (or absence) of decompensating events, and validated prognostic tools. [1] [2] [6]
In this story, “stage” is not a moral label. It is clinical shorthand for what the liver can still do, what it can no longer do, and what must be watched for next. “Compensated” cirrhosis means the liver is scarred but still maintaining relative stability; “decompensated” means complications such as ascites, variceal bleeding, encephalopathy, jaundice, or renal dysfunction have appeared—and prognosis changes meaningfully at that inflection point. [6] [7]
MELD is used in U.S. allocation because it is a lab-based model tied to near-term mortality risk in advanced disease, while Child–Pugh remains useful for clinical framing because it includes ascites and encephalopathy—two variables that can dominate day-to-day life. [8] [9] [10]
Stage 1: Quiet Injury
At first, the liver is generous. The alcohol patient may feel “fine” between binges; the MASLD/MASH patient may only see mildly elevated enzymes; the viral hepatitis patient may have years of low-grade inflammation; the autoimmune patient may fluctuate between flares and calm. This early chapter is often clinically silent—sometimes reversible—if the primary driver is removed or controlled early. [1] [2] [3] [5]
The plot twist is that symptoms are a poor narrator. Many patients feel little until substantial scarring has already accumulated. That is why clinicians rely on objective markers—history, labs, fibrosis assessment with noninvasive tests (including elastography), and sometimes biopsy—to determine whether this “quiet” chapter is truly mild or merely silent. [2] [11]
Stage 2: Fibrosis
Fibrosis is the liver’s attempt to heal—collagen laid down like scaffolding after repeated injury. Over time, that scaffolding can become a cage. Mechanistically, chronic injury activates fibrogenic pathways (including hepatic stellate cell activation and extracellular matrix deposition), increasing resistance to blood flow and setting the stage for portal hypertension. [11] [7]
Etiology shapes tempo. Continued heavy alcohol use can accelerate progression; MASLD/MASH progression is strongly influenced by metabolic drivers; viral hepatitis outcomes improve dramatically with effective antiviral therapy; and autoimmune hepatitis progression is reduced by appropriate immunosuppression and maintenance strategies. [1] [2] [3] [4] [5]

Here, the story becomes measurable. Pathology staging systems and noninvasive tests help describe scar burden, and repeated assessment can help track change over time. This is the chapter where early, sustained interventions can materially change the ending. [2]
Stage 3: Cirrhosis
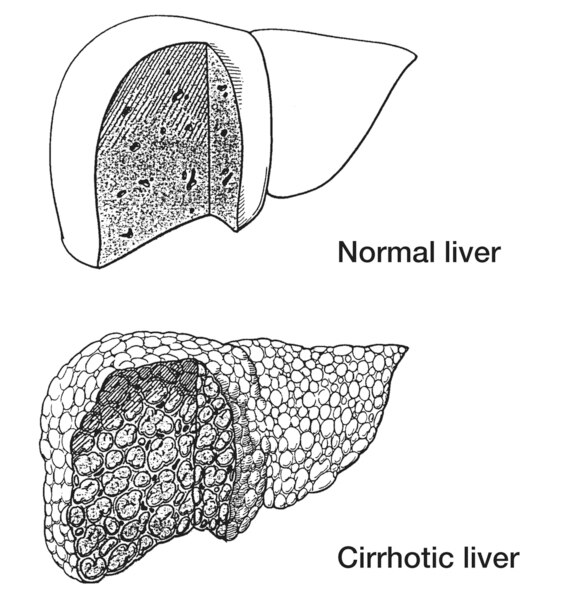
Cirrhosis is when scar becomes architecture: nodules boxed in by fibrous bands, with reduced functional reserve and rising portal pressure. Some cirrhosis remains “compensated,” meaning major complications have not yet appeared—even though risk is now real and surveillance becomes central. [6] [7]
This chapter introduces prevention as a lead character: risk stratification for portal hypertension and varices, plus strategies to reduce the chance of first decompensation and manage bleeding risk. Many transplant evaluations begin in this chapter—before crisis forces the timing. [7]
The four patients now begin to resemble each other clinically. The etiology still matters—but the shared physiology of portal hypertension and reduced synthetic function starts to dominate planning, surveillance, and risk. [6]
Stage 4: Decompensation
Decompensation is the turning point most patients remember: ascites that will not stay controlled, variceal bleeding, encephalopathy, jaundice, or kidney dysfunction. After decompensation, near-term risk rises sharply, and timing conversations (including transplant evaluation and listing strategy) become more urgent. [6] [7]
This is where MELD becomes the clock the transplant system listens to, because it uses lab inputs tied to mortality risk. Child–Pugh continues to matter clinically because it explicitly incorporates ascites and encephalopathy—two complications that can be decisive in real-world functioning even when MELD is “not that high.” [8] [9] [10]
MELD & Child–Pugh: Why Two Scores Exist
MELD was developed as a model to predict short-term mortality in advanced liver disease and became central to allocation frameworks because it supports an objective, lab-driven prioritization process. In OPTN patient resources, MELD is described as a calculated formula used to assign priority for most adult liver transplant candidates, using specified lab inputs. [8] [9]
Child–Pugh persists because it narrates something MELD does not directly encode: the lived burden of ascites and encephalopathy—alongside bilirubin, INR (or prothrombin time), and albumin. The modern framework traces to Pugh’s modification of earlier surgical risk classification work in cirrhosis. [10]
In story terms: MELD estimates urgency; Child–Pugh describes how hard the days are. Many care decisions use both—one to prioritize, the other to contextualize. [8] [10]
Tables
MELD vs Child–Pugh (Side-by-Side)
| Feature | MELD | Child–Pugh |
|---|---|---|
| Purpose | Predicts short-term mortality risk in advanced disease; used in allocation frameworks. [8] [9] | Clinical severity framing including ascites/encephalopathy. [10] |
| Inputs | Model uses lab inputs specified in the original and subsequent implementations (allocation versions are lab-based). [8] [9] | Bilirubin, albumin, INR/prothrombin time, ascites, encephalopathy. [10] |
| Strengths | Objective, reproducible, lab-driven. [8] [9] | Captures symptomatic decompensation burden. [10] |
| Limitations | Does not directly encode ascites/encephalopathy burden. [10] | Partly subjective (grading ascites/encephalopathy); not designed for allocation. [10] |
Practical reading: MELD is the transplant “urgency number,” while Child–Pugh is the clinical “how decompensated is this patient” narrative. Many transplant teams use both lenses in parallel. [8] [10]
Stage-by-Stage Markers (Etiology-Aware, Typical—not Absolute)
| Stage | Story marker | Alcohol-associated liver disease | MASLD/MASH | Viral hepatitis (HBV/HCV) | Autoimmune hepatitis |
|---|---|---|---|---|---|
| Stage 1 Quiet injury |
Symptoms unreliable; labs/imaging may be subtle. | Steatosis/steatohepatitis risk; sustained abstinence changes trajectory. [1] | Steatosis ± inflammation; metabolic management matters early. [2] | Chronic inflammation can be silent; modern guidance emphasizes testing and treatment pathways. [3] [4] | Flares and remission; guideline-based therapy reduces progression risk. [5] |
| Stage 2 Fibrosis |
Scar accumulates; noninvasive fibrosis assessment becomes meaningful. | Progression accelerated by ongoing heavy use and related factors. [1] | Progression risk stratification is central to care pathways. [2] | Antiviral therapy improves long-term outcomes and reduces progression risk. [3] [4] | Undertreated disease can progress; maintenance strategies are emphasized in guidelines. [5] |
| Stage 3 Compensated cirrhosis |
Architectural distortion; portal hypertension risk increases; surveillance and prevention lead. | Risk shifts toward portal-hypertension complications; prevention strategies apply. [7] | Portal hypertension and fibrosis stage drive monitoring intensity and referral planning. [2] | HBV/HCV guidance supports pathways that change outcomes; surveillance/prevention remain essential once cirrhosis exists. [3] [4] | Guidelines emphasize diagnosis, therapy, and long-term management to prevent progression and complications. [5] |
| Stage 4 Decompensated cirrhosis |
Ascites/bleeding/HE/jaundice/renal dysfunction; transplant urgency rises. | Decompensation events sharply change prognosis; management focuses on preventing/reducing complications. [6] [7] | Symptom burden may be high; Child–Pugh helps describe ascites/HE impact. [10] | MELD-based allocation discussions often intensify once decompensation occurs; antiviral therapy still matters but cannot guarantee reversal of portal hypertension. [3] [9] | Decompensation plus uncontrolled inflammation can accelerate; specialist management is essential. [5] |
These markers are intentionally labeled “typical” because etiology changes tempo, and intercurrent events (bleeding, infection, kidney injury) can shift severity quickly. The safest use is as a conversation starter: “Which row am I in—and what would push me into the next chapter?” [6]
Questions to Ask Your Liver or Transplant Team
- In your view, am I compensated or decompensated—and what single complication would change my risk the most? [6]
- Which etiology is driving my disease now—alcohol, MASLD/MASH, viral hepatitis, autoimmune hepatitis, or more than one—and how does that change the plan? [1] [2] [5]
- What is my current MELD, and what specific events would make it rise quickly? [9]
- What is my Child–Pugh class, and how much is driven by ascites or encephalopathy versus labs? [10]
- What portal-hypertension prevention or surveillance do I need now (including bleeding risk strategies), and how often? [7]
- If transplant is on the horizon, what are the triggers for referral, evaluation, and listing in my case? [9]
References
- Crabb DW, Im GY, Szabo G, et al. (AASLD Practice Guidance; PubMed PMID: 31314133). Diagnosis and Treatment of Alcohol-Associated Liver Diseases (Hepatology, 2020).
- Rinella ME, et al. (AASLD Practice Guidance; PubMed PMID: 36727674). Clinical assessment and management of nonalcoholic fatty liver disease (Hepatology, 2023).
- Bhattacharya D, et al. (AASLD-IDSA Guidance Update; PubMed PMID: 37229695). Hepatitis C Guidance 2023 Update: testing, managing, and treating HCV infection.
- Terrault NA, Lok ASF, McMahon BJ, et al. (AASLD Guidance; PubMed PMID: 29405329). Prevention, diagnosis, and treatment of chronic hepatitis B (Hepatology, 2018).
- European Association for the Study of the Liver (EASL). (PubMed PMID: 26341719). EASL Clinical Practice Guidelines: Autoimmune hepatitis (J Hepatol, 2015).
- D’Amico G, Garcia-Tsao G, Pagliaro L. (PubMed PMID: 16298014). Natural history and prognostic indicators of survival in cirrhosis: systematic review (J Hepatol, 2006).
- Kaplan DE, et al. (AASLD Practice Guidance; PubMed PMID: 37870298). Risk stratification and management of portal hypertension and varices in cirrhosis (Hepatology, 2024).
- Kamath PS, Wiesner RH, Malinchoc M, et al. (PubMed PMID: 11172350). Model for End-Stage Liver Disease (MELD) to predict survival in end-stage liver disease (Hepatology, 2001).
- OPTN/HRSA (Official). Learn about MELD (OPTN allocation calculator resource).
- Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. (PubMed PMID: 4541913). Transection of the oesophagus for bleeding oesophageal varices (Br J Surg, 1973) — foundation of the Child–Pugh framework.
- Bataller R, Brenner DA. (JCI). Liver fibrosis (Figure 1; mechanisms and architectural change).
- NIDDK/NIH Media Library. “Cirrhosis Reality” media asset (image credit: NIDDK/NIH).
- NIDDK/NIH Media Library. “Portions of normal and cirrhotic liver tissues” media asset (image credit: NIDDK/NIH).