
High Altitude Sickness (AMS) and Liver Disease to Transplant
High Altitude Sickness—also called Acute Mountain Sickness (AMS)—can occur after rapid ascent (often > ~8,000 ft / 2,500 m) when the body has insufficient time to acclimatize to lower oxygen pressure [1][2]. For patients with advanced liver disease or liver transplant recipients, hypoxia and altitude-related fluid shifts may be harder to tolerate due to anemia, cardiopulmonary complications of cirrhosis (e.g., hepatopulmonary syndrome or portopulmonary hypertension), and post-transplant comorbidities (e.g., kidney dysfunction, hypertension) [6][7][8].
- Prevention first: staged ascent + rest days reduce AMS risk.
- New confusion matters: at altitude it could be AMS/HACE, infection, medication effect, or hepatic encephalopathy—do not “tough it out.”
- Shortness of breath at rest is a red flag: consider HAPE, cardiopulmonary disease, or anemia—seek urgent care.
- Medication plans require coordination: acetazolamide and dexamethasone have specific risks, especially with renal dysfunction.
What Is High Altitude Sickness?
As elevation increases, barometric pressure falls, lowering the amount of oxygen available with each breath (hypobaric hypoxia). If ascent is too rapid, the body may not acclimatize in time, resulting in AMS [1][2].
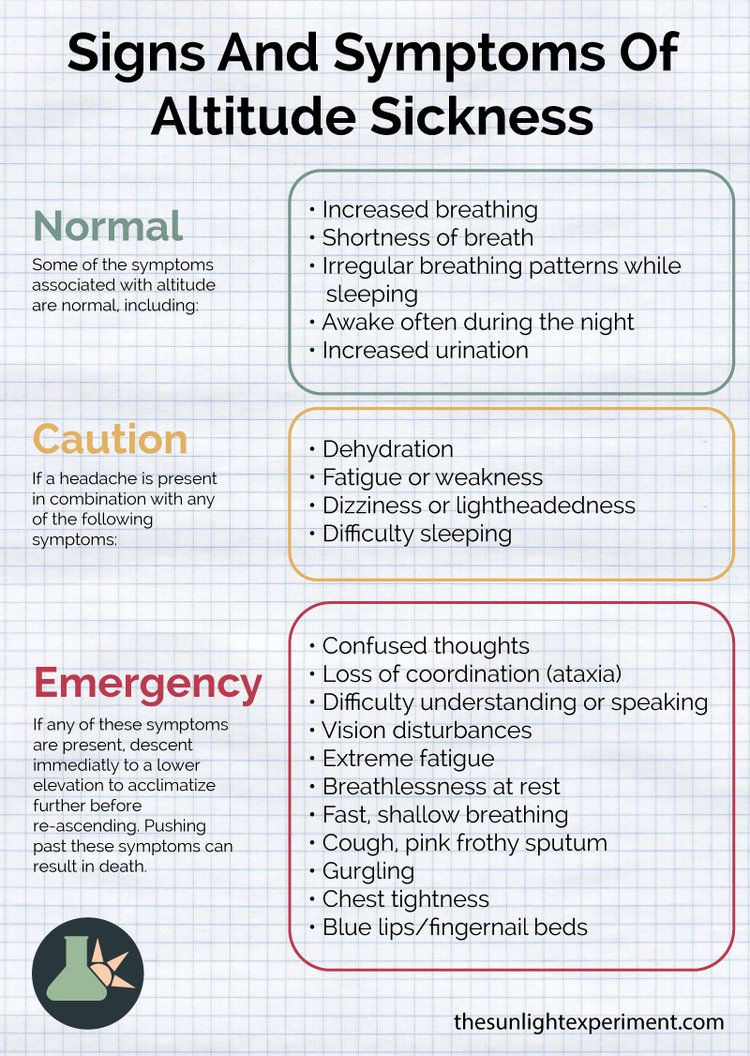
Symptoms and Severity Spectrum
Early AMS symptoms often resemble dehydration, exhaustion, flu, or a hangover, typically starting within hours of arrival or exertion at altitude. Classic features include headache plus nausea, fatigue, dizziness, and sleep disturbance [2][3].
Mild AMS
- Headache, fatigue/weakness, dizziness/lightheadedness
- Nausea, decreased appetite
- Difficulty sleeping
Moderate AMS
- Worsening headache not responding to simple measures
- Repeated vomiting
- Marked fatigue, shortness of breath with minimal activity
- Unsteadiness (ataxia) or impaired coordination
Severe altitude illness (Emergency)
- HACE: confusion, inability to walk straight, severe lethargy, possible loss of consciousness
- HAPE: breathlessness at rest, cough, chest tightness, frothy/pink sputum, bluish lips/fingernails
Diagnosis and Medical Workup
Diagnosis is primarily clinical: recent ascent + compatible symptoms. The Lake Louise symptom-based criteria are widely used to grade AMS severity [3]. Pulse oximetry can support assessment but does not replace clinical judgment.
In severe cases or diagnostic uncertainty, clinicians may evaluate for pneumonia, pulmonary embolism, heart failure, medication effects, or neurologic causes. Imaging (chest X-ray for suspected HAPE; brain imaging if severe neurologic symptoms) is typically reserved for complicated cases [4].
Pathophysiology
Hypobaric hypoxia triggers hyperventilation and a cascade of vascular and inflammatory responses. AMS is thought to involve altered cerebral blood flow, neurohormonal changes, and increased capillary permeability. When severe, these responses can progress to cerebral edema (HACE) or non-cardiogenic pulmonary edema (HAPE) [2][4].
Why Liver Disease Can Increase Altitude Risk
Advanced liver disease can reduce physiologic reserve. Several cirrhosis-related conditions may be particularly relevant at altitude:
- Anemia and malnutrition may reduce oxygen delivery and exercise tolerance.
- Hepatopulmonary syndrome (HPS) causes impaired oxygenation and may worsen dyspnea/hypoxemia in low-oxygen environments [7].
- Portopulmonary hypertension (PoPH) can limit cardiopulmonary response to hypoxia and exertion [8].
Special Considerations After Liver Transplant
Post-transplant patients often do very well with travel, but altitude planning should be individualized. Issues to discuss with your transplant team include:
- Kidney function: acetazolamide dosing and safety are affected by renal impairment [2].
- Hypertension/fluid balance: altitude-related physiologic stress plus immunosuppression-associated hypertension may worsen symptoms.
- Infection risk: respiratory infections can mimic or worsen altitude illness; seek early evaluation when sick.
- Medication interactions and side effects: sedation, dizziness, and nausea can confound symptom interpretation.
Prevention (Most Important)
Prevention centers on graded ascent, allowing acclimatization time. General guidance includes limiting daily sleeping-elevation gains and adding rest days [2]. Avoid heavy exertion and alcohol early after arrival; maintain hydration and nutrition.
Treatment Options
The first-line treatment for worsening AMS is descent. Supplemental oxygen helps reverse hypoxia when descent is delayed. Medications may be used depending on severity and clinical context: [2][4]
- Acetazolamide: can aid acclimatization; dosing must consider renal function and clinician guidance.
- Dexamethasone: used for severe AMS/HACE features while arranging descent/evacuation.
- HAPE therapies: oxygen + descent; specific agents (e.g., nifedipine) may be considered under medical direction.
- Portable hyperbaric bag: may be used when descent is not immediately possible.
When It’s an Emergency
Do not stay at altitude (and do not ascend) if any of the following occur: [2]
- Confusion, ataxia, inability to walk straight, severe drowsiness (possible HACE)
- Breathlessness at rest, cyanosis, frothy/pink sputum, gurgling chest sounds (possible HAPE)
- Chest pain, fainting, or rapidly worsening symptoms
References
- CDC — Travel to High Altitudes (altitude illness overview, prevention, and safety)
- Wilderness Medical Society Clinical Practice Guidelines — Prevention and Treatment of Acute Altitude Illness (PubMed)
- Lake Louise AMS Consensus (2018 update) — diagnostic criteria framework (PubMed)
- StatPearls (NCBI Bookshelf) — High Altitude Illness (clinical features, diagnosis, and management)
- StatPearls (NCBI Bookshelf) — Cirrhosis and associated systemic complications (clinical context)
- StatPearls (NCBI Bookshelf) — Hepatopulmonary Syndrome (hypoxemia risk in cirrhosis)
- StatPearls (NCBI Bookshelf) — Portopulmonary Hypertension (cardiopulmonary limitation in portal HTN)