
Gastric Bypass & Liver Transplantation
Morbid obesity is increasingly common in liver transplant candidates, often worsening NAFLD/NASH and complicating surgery. Gastric bypass (RYGB) can be a game-changer for weight loss and liver health — before, during, or after transplant. This page covers timing, benefits, risks, and evidence-based guidance.
Obesity in Liver Transplant Candidates
Over 40% of U.S. liver transplant waitlist patients have BMI >30, with morbid obesity (BMI >40) disqualifying up to 20% from listing due to surgical risks like wound infections and technical difficulties. NAFLD/NASH, driven by obesity, now causes 25–30% of transplants. Without intervention, post-transplant weight gain recurs in 60–70%, risking graft steatosis.[1]
Benefits of Gastric Bypass for Liver Health
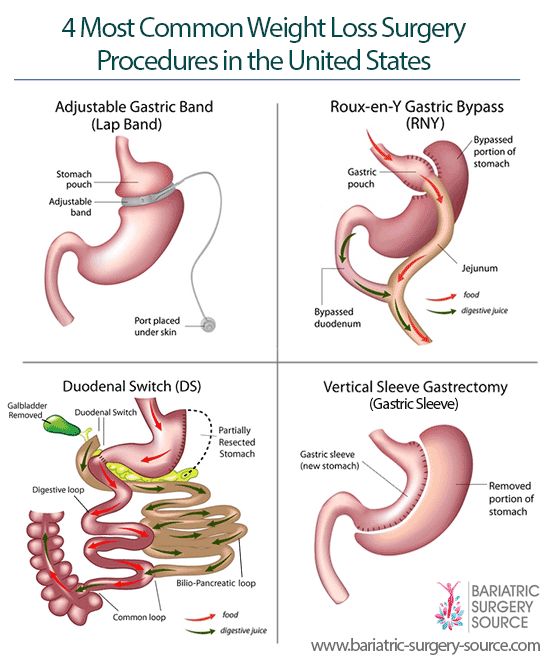
Roux-en-Y gastric bypass (RYGB) induces 60–70% excess weight loss, resolving NASH in 70–85% and improving fibrosis. It corrects metabolic syndrome (diabetes remission 70–80%, hypertension 50%), reducing cardiovascular risks critical post-transplant. RYGB also stabilizes portal hypertension, potentially lowering variceal bleed risk in cirrhotics.[2]
Pre-Transplant Gastric Bypass
RYGB before listing achieves BMI <35 in 80% within 12–18 months, enabling eligibility. In NAFLD patients, it reverses steatosis and improves MELD scores by enhancing liver function. Risks include malnutrition worsening cirrhosis (10–15%), but benefits outweigh in stable candidates. Centers recommend multidisciplinary evaluation; success rates >90% for weight goals.[3]
Simultaneous Liver Transplant & Bypass
Combined procedures (e.g., sleeve gastrectomy with LT) are safe in high-volume centers, with no increased mortality vs LT alone. Mayo Clinic data shows sustained weight loss (BMI drop 15–20 points at 5 years), diabetes resolution (80%), and no NASH recurrence. Operative time increases 1–2 hours, but hospital stays match standard LT.[4]
Post-Transplant Gastric Bypass
RYGB after LT is feasible 6–12 months post-op, with 50–60% excess weight loss and NASH regression in recurrent cases. Complications (leaks 5%, infections 10%) are higher due to adhesions/immunosuppression, but long-term graft survival improves. Ideal for patients regaining >20 kg post-LT; laparoscopic approach preferred.[5]
Risks & Complications
Perioperative risks include anastomotic leaks (2–5%), malnutrition exacerbating sarcopenia (15%), and interactions with immunosuppression (tacrolimus malabsorption). In cirrhotics, portal hypertension raises bleed risk (10%). Overall mortality <1% in experienced hands; close monitoring essential for vitamin deficiencies common in RYGB.[3]
Nutritional Management Post-Bypass
Post-RYGB, protein intake (1.2–1.5 g/kg) prevents muscle loss; multivitamins, B12, iron, calcium mandatory lifelong. In transplant patients, adjust for steroid-induced catabolism. Dietitians tailor plans; dumping syndrome affects 20–30%, but resolves with education. Liver function improves with weight loss, reducing encephalopathy risk.[2]
Patient Selection & Timing
Select stable MELD <25 patients without active decompensation; avoid in severe portal hypertension. Pre-LT RYGB for BMI >40; simultaneous for BMI 35–40 with NASH; post-LT for weight regain >15%. Multidisciplinary teams (hepatology, bariatrics, nutrition) optimize outcomes; 85% achieve transplant eligibility post-bypass.[1]
References
- Heimbach JK, et al. Combined liver transplantation and gastric sleeve resection for patients with medically complicated obesity and end-stage liver disease. Am J Transplant 2013;13(2):363-368.
- Marchesini G, et al. Roux-en-Y gastric bypass for recurrent nonalcoholic steatohepatitis in liver transplant recipients with morbid obesity. Hepatology 2001;34(1):155-158.
- Abu Dayyeh BK, et al. Gastric bypass after liver transplantation. Obes Surg 2014;24(2):185-193.
- Mayo Clinic News Network. Study finds long-term health benefits from bariatric surgery and liver transplant. 2025 Jun 2.
- Sanyal A, et al. Laparoscopic Roux-en-Y gastric bypass is safe and feasible after orthotopic liver transplantation. Obes Surg 2005;15(12):1668-1672.