
BMI & BMR in Liver Transplant Patients
Body Mass Index (BMI) and Basal Metabolic Rate (BMR) help frame nutritional status before and after liver transplantation, but in cirrhosis they can be misleading due to ascites/edema and sarcopenia [4][7]. This page includes calculators and liver-disease–specific interpretation.
Body Mass Index (BMI) Explained
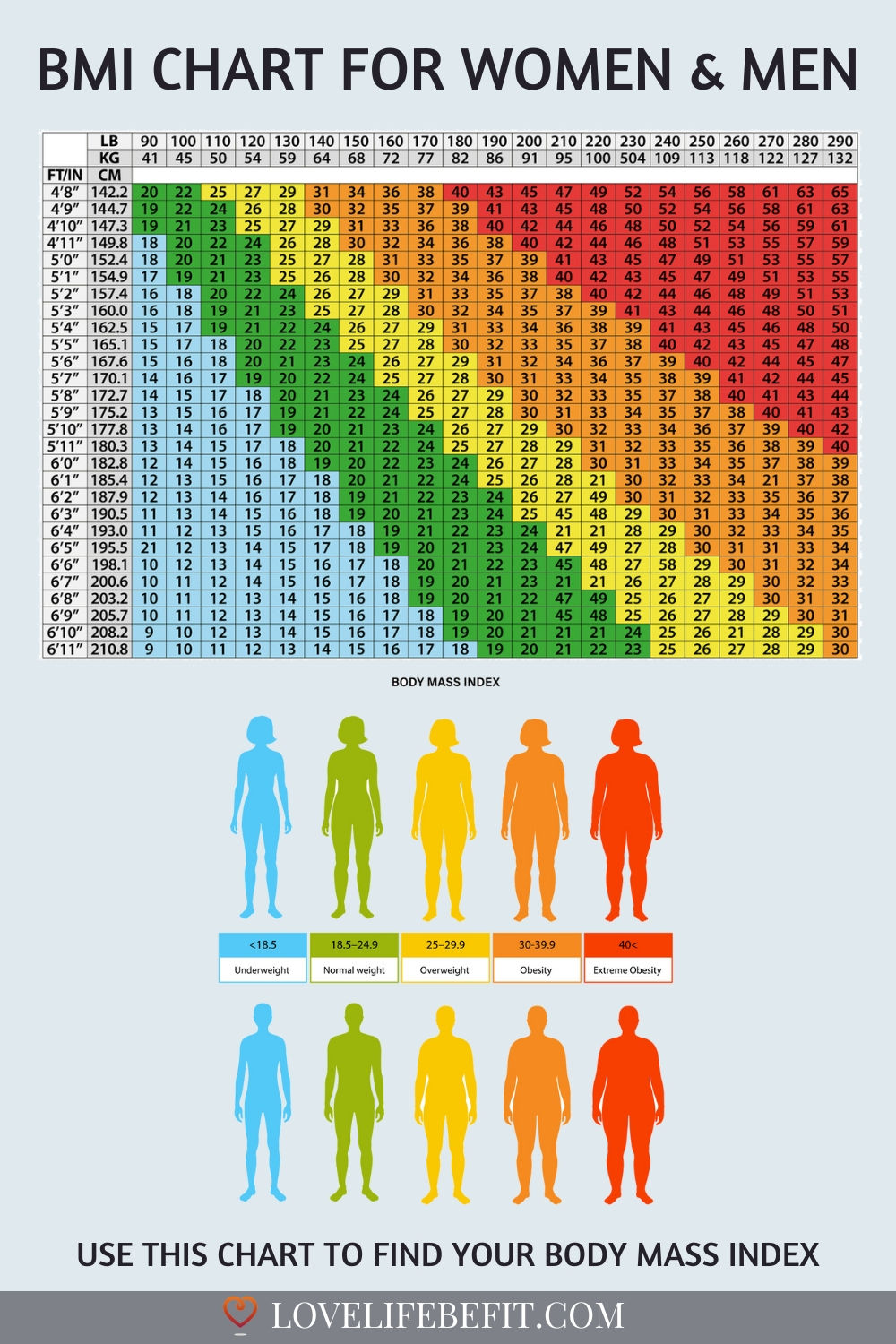
Definition: BMI is a weight-for-height screening metric: BMI = weight (kg) ÷ [height (m)]², or BMI = weight (lb) ÷ [height (in)]² × 703 [2].
Categories: <18.5 underweight | 18.5–24.9 normal | 25–29.9 overweight | ≥30 obese [1].
Why BMI can mislead in cirrhosis: ascites and edema can falsely elevate weight, while sarcopenia (muscle loss) can mask malnutrition even at “normal” or high BMI—often termed “sarcopenic obesity,” which is associated with worse outcomes [4][5].
BMI Calculator (Liver-Disease Aware)
Calculate BMI
Basal Metabolic Rate (BMR) Explained
BMR is the energy (calories) your body requires at complete rest. In clinical practice, the Mifflin–St Jeor equation is commonly used to estimate resting energy expenditure [6].
Why BMR estimates can be off in cirrhosis: some patients are hypermetabolic (measured needs exceed predicted), while others may be hypometabolic. Nutrition plans should be individualized and adjusted based on weight trend, intake tolerance, muscle status, and clinical course [7].
BMR & Daily Calorie Needs Calculator
Estimate BMR and Daily Needs (TDEE)
Special Considerations in Liver Disease & Transplantation
- Fluid overload inflates weight: BMI may overestimate adiposity when ascites/edema is present [4].
- Sarcopenia matters: muscle loss can coexist with overweight/obesity (“sarcopenic obesity”) and is linked to worse outcomes [4][5].
- Nutrition targets are often higher: common cirrhosis targets include ~35–40 kcal/kg/day and 1.2–1.5 g protein/kg/day (dry weight), individualized by your transplant dietitian/team [7][8].
- Post-transplant weight gain is common: improved appetite and some immunosuppressants can accelerate weight gain—early counseling helps [8].
Medical Disclaimer
These calculators are for education only. In cirrhosis and after liver transplantation, BMI and BMR estimates may not reflect true nutritional status. Review results with your hepatologist and transplant nutrition team.
References
- CDC. Adult BMI Categories. Verified link
- CDC. Adult BMI Calculator (method and interpretation). Verified link
- NHLBI. BMI Tools. Verified link
- EASL Clinical Practice Guidelines: nutrition in chronic liver disease (J Hepatol 2019). PubMed
- Sarcopenic obesity in cirrhosis (European registry study) — J Hepatol 2023. PubMed
- Mifflin MD et al. Predictive equation for resting energy expenditure. Am J Clin Nutr 1990. PubMed
- ESPEN practical guideline: Clinical nutrition in liver disease. Clin Nutr 2020. PubMed
- AASLD. Long-Term Management of the Adult Liver Transplant (guideline page). Verified link