
Hernias Post Liver Transplantation: Diabetes, A1C, and Wound Healing
Abdominal wall hernias—especially incisional hernias—are a recognized long-term complication after liver transplantation [4][5]. Diabetes and hyperglycemia can impair healing via microvascular dysfunction, immune impairment, and abnormal collagen/repair biology [9]. This page explains types of hernias, how they are diagnosed, and how A1C and immunosuppression influence wound durability.
- Most common: incisional hernia at the transplant incision site.
- Red flags: severe pain, vomiting, skin color change over the bulge, or inability to reduce the hernia (possible incarceration/strangulation).
- Diabetes matters: hyperglycemia can raise infection risk and weaken repair biology, impacting wound durability.
- Immunosuppression matters: certain regimens (notably mTOR inhibitors in some contexts) are associated with wound-healing complications.
Introduction and Historical Context
Liver transplantation evolved from an experimental procedure into standard life-saving therapy through decades of innovation. Dr. Thomas Starzl is widely credited as a foundational pioneer; long-term survival after liver transplant became feasible in the late 1960s as surgical technique and immunosuppression advanced [3].
As survival improved, attention shifted toward long-term complications. One important category is the development of abdominal wall hernias— most commonly incisional hernias at prior surgical sites [4].
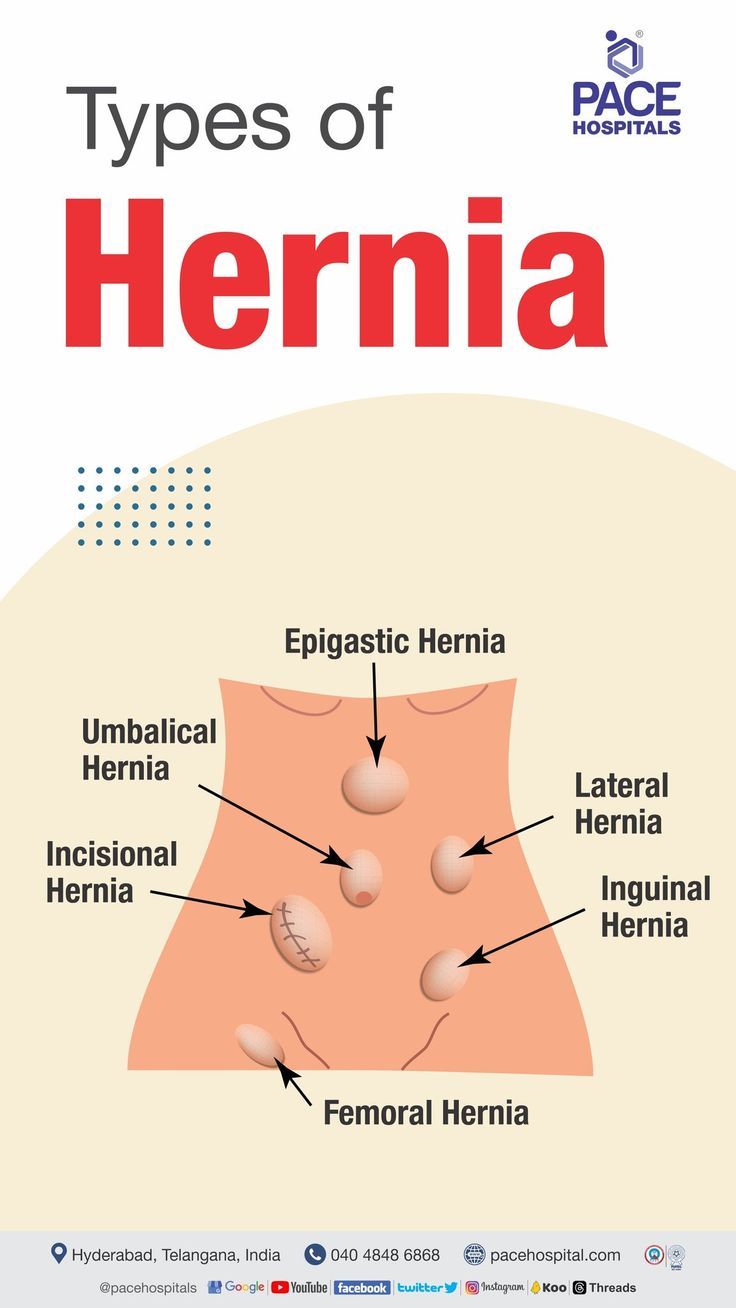
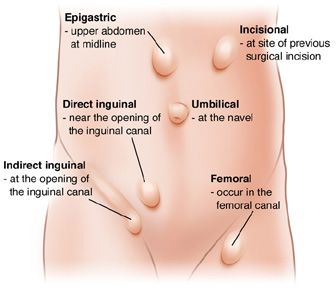
Types of Hernias After Liver Transplant
A hernia occurs when internal tissue bulges through a weak area in the abdominal wall [2]. After liver transplant, hernias may include:
- Incisional hernia: through the transplant incision or scar (most common in this setting) [4].
- Internal hernia: inside the abdominal cavity (often related to internal anatomy/adhesions; diagnosis is imaging-driven).
- Umbilical hernia: at the navel, sometimes pre-existing and sometimes worsened by ascites/abdominal wall weakness [2].
- Parastomal hernia: around a stoma (uncommon after liver transplant unless an ostomy exists).
Incidence and Typical Location
Reported rates vary by center, incision type, and follow-up duration. Reviews in liver transplant recipients report incisional hernia rates that commonly fall in the low-to-mid teens on average, with wider ranges reported across studies [5][7].
Clinical Presentation and Diagnosis
Many patients notice a bulge near an incision that becomes more prominent with standing, coughing, or straining. Discomfort may range from pressure to pain. Some hernias are discovered incidentally on imaging.
- Visible or palpable bulge near the scar
- Aching/pressure worsened by activity or lifting
- Occasional nausea or constipation (especially if bowel is involved)
Clinical exam is often sufficient, but imaging is frequently used to define anatomy and plan repair. Ultrasound can confirm a hernia in many settings, and CT is often used for complex abdominal wall cases or preoperative planning.
The Diabetes Factor in Wound Healing
Diabetes can impair wound healing through microvascular dysfunction and reduced tissue oxygenation, impaired immune response, and dysregulated inflammatory and repair phases [9]. These effects can increase susceptibility to infection and weaken tissue repair—both of which matter for fascial strength after a large abdominal incision.
Understanding A1C and Why It Matters
Hemoglobin A1C (HbA1c) estimates average glucose over ~2–3 months. In surgical populations, poorer glycemic control is associated with higher postoperative infectious complication rates; one large study reported lower infection risk with HbA1c < 7% [10]. Other analyses suggest risk can rise even in the 6–7% range for some abdominal surgery complications [11].
Immunosuppression and Wound Healing
Immunosuppression is essential for graft survival, but it can complicate wound healing by increasing infection risk and altering tissue repair pathways. Reviews note that mTOR inhibitors (e.g., sirolimus/everolimus) have been associated with wound-healing complications in transplant populations [12][14].
Risk Reduction and Prevention Strategies
Risk reduction focuses on optimizing modifiable factors (glucose/A1C when feasible, nutrition, weight, pulmonary status) and careful planning around immunosuppression for elective repair [7][15].
Treatment Options and Surgical Approaches
Options include observation (selected cases) and surgical repair. Repair approach (open, laparoscopic, robotic) and technique (primary closure vs mesh) depend on hernia size, symptoms, and patient risk factors. Reviews focused on liver transplant recipients emphasize individualized decision-making and coordination with the transplant team [15].
When It’s Urgent: Red Flags
- Severe, escalating pain at the hernia site
- Vomiting, inability to pass gas, or abdominal distension
- Skin discoloration over the bulge (red/purple/dusky), fever
- Non-reducible hernia (cannot gently push it back when lying down)
References
- MedlinePlus (NIH). Hernia (overview, including incisional and umbilical types) .
- VA Research. First successful liver transplant (Starzl; historical context) .
- Smith CT, Katz MG, Foley D, et al. Incisional hernias after transplantation (risk factors overview) . (PubMed Central).
- Butler JR, et al. Incisional hernia after orthotopic liver transplantation (meta-analysis summary) . (ScienceDirect).
- Kannan SS, et al. Incisional hernia repair following liver transplantation (management overview) . World Journal of Transplantation.
- Spampinato SF, Caruso GI, De Pasquale R, et al. Impaired wound healing in diabetes (mechanisms) . (PubMed Central).
- Dronge AS, Perkal MF, Kancir S, et al. Long-term glycemic control and postoperative infectious complications (HbA1c threshold context) . JAMA Surgery.
- Wong JKL, et al. Preoperative HbA1c and postoperative complications (abdominal surgery risk signals) . (PubMed Central).
- Khalil MAM, et al. mTOR inhibitors and wound-healing complications in transplantation (review) . (PubMed Central).
- Campistol JM, et al. Practical recommendations for early use of mTOR inhibitors (wound-healing considerations) (PDF) .
- Ayuso S, et al. Management of incisional hernias in liver transplant patients (overview) . (LWW).