
Ascites and Liver Disease
Ascites is one of the most common and life-altering complications of advanced cirrhosis. It typically reflects clinically significant portal hypertension and is associated with higher risks of infection (including spontaneous bacterial peritonitis) and kidney dysfunction [1][2][4]. For many patients, the onset of clinically significant or recurrent ascites is a key trigger for urgent transplant evaluation [1][3].
What Is Ascites?
Ascites is the abnormal accumulation of fluid in the peritoneal cavity. In cirrhosis, it usually results from portal hypertension and circulatory changes that activate neurohormonal systems and cause the kidneys to retain sodium and water [1][2]. Symptoms often include abdominal distension, early satiety, reflux, weight gain from fluid (not fat), and shortness of breath—especially when ascites becomes tense [2].
Clinicians often describe ascites as: grade 1 (only visible on imaging), grade 2 (moderate symmetrical abdominal distension), and grade 3 (large or tense ascites) [1][2].
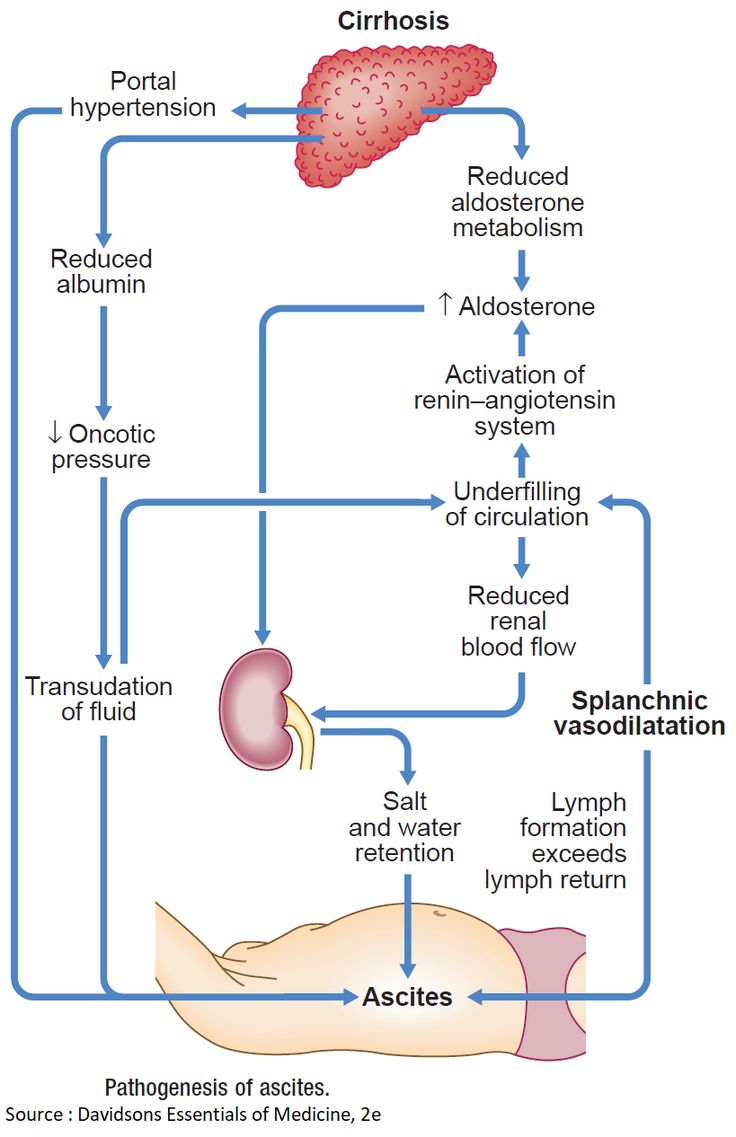
Why Ascites Develops in Cirrhosis
Portal hypertension promotes dilation of blood vessels in the splanchnic (abdominal) circulation. This lowers “effective” arterial blood volume, activating the renin–angiotensin–aldosterone system (RAAS), sympathetic nervous system, and vasopressin (ADH). The net effect is renal sodium and water retention and expansion of plasma volume—yet fluid preferentially shifts into the peritoneal cavity due to altered pressures and permeability [1][2].
As disease progresses, ascites may become refractory (poorly responsive to diuretics). Refractory ascites is associated with higher rates of acute kidney injury and hepatorenal syndrome, and it often signals clinical deterioration [2][3].
Symptoms and Impact on Daily Life
Ascites can cause abdominal discomfort, difficulty bending, early fullness after meals (which can worsen malnutrition), reflux, and breathlessness (especially when lying flat). Frequent hospital visits, repeated paracenteses, and the fear of infection can be emotionally draining [2][5].
Major complications include:
- Spontaneous bacterial peritonitis (SBP): a potentially life-threatening infection of ascitic fluid [2].
- Kidney dysfunction (AKI/HRS): often precipitated by infection, over-diuresis, dehydration, or severe circulatory dysfunction [2][3].
- Malnutrition and sarcopenia: worsened by early satiety and reduced physical activity [1][5].
Treatment, Paracentesis, and TIPS
Management is stepwise and must be individualized:
- Sodium restriction: typically a low-sodium diet (often ~2 g/day sodium, individualized) to reduce fluid accumulation [1][2].
- Diuretics: commonly spironolactone with or without furosemide, titrated carefully to avoid kidney injury and electrolyte shifts [2].
- Large-volume paracentesis (LVP): standard for tense or refractory ascites; albumin is commonly recommended when removing large volumes to reduce circulatory dysfunction [2].
- TIPS: may improve ascites control in selected patients; risks (especially encephalopathy) must be weighed carefully [6][7].
Many patients use serial paracenteses as a bridge to transplant. Your team will watch kidney function, sodium, potassium, blood pressure, and encephalopathy symptoms closely during treatment [2][3].

Ascites and Timing of Transplant Evaluation
Clinically significant, recurrent, or refractory ascites should prompt discussion of transplant evaluation and listing strategy. Ascites is a marker of decompensation and is associated with increased mortality risk in cirrhosis, especially when complicated by SBP or kidney dysfunction [1][2][3].
After successful liver transplantation, ascites typically resolves as portal hypertension and liver synthetic function normalize [8].
Medical Disclaimer
This page is educational only and does not replace medical advice. Ascites management (diuretics, paracentesis, albumin, TIPS, antibiotic prophylaxis, and transplant timing) must be directed by your hepatologist and transplant team [2][1]. Seek urgent care for fever, severe abdominal pain/tenderness, confusion, fainting, black or bloody stools, vomiting blood, or sudden worsening.
References
- EASL. Clinical Practice Guidelines for the management of patients with decompensated cirrhosis (J Hepatol 2018 – full text). Full text | PubMed
- AASLD. Diagnosis, Evaluation, and Management of Ascites, SBP, and Hepatorenal Syndrome (Practice Guidance; updated Aug 2021). AASLD Guidance page | PubMed
- Angeli P, et al. Consensus/recommendations on AKI in cirrhosis (includes HRS concepts; PubMed). PubMed
- Runyon BA, et al. Management of adult patients with ascites due to cirrhosis (AASLD practice guideline update – PubMed). PubMed (2009 update)
- Quality of life and symptom burden in cirrhosis with ascites (PubMed record as provided). PubMed
- EASL Clinical Practice Guidelines on TIPS (full text). Full text
- TIPS vs repeated large-volume paracentesis / refractory ascites evidence review (PubMed record as provided). PubMed
- Resolution of ascites after liver transplantation (PubMed record as provided). PubMed