
Cirrhosis and Liver Transplantation
A comprehensive guide to understanding cirrhosis, its complications, and the pathway to liver transplantation.
Understanding Cirrhosis
Cirrhosis represents the irreversible end-stage of chronic liver injury, characterized by widespread fibrosis, nodule formation, and architectural distortion. These changes impair portal blood flow, reduce functional hepatocyte mass, and disrupt detoxification, protein synthesis, and metabolic regulation. Leading etiologies include metabolic dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD/NASH), chronic viral hepatitis B/C, alcohol-related liver disease, autoimmune conditions, and genetic disorders such as hemochromatosis or Wilson disease. Multifactorial injury is common. Clinically, cirrhosis progresses from compensated (asymptomatic) to decompensated phases marked by ascites, variceal bleeding, encephalopathy, or jaundice—events that dramatically worsen prognosis and often trigger transplant evaluation. Tools like Child–Pugh and MELD-Na scores quantify severity and guide urgency of referral.[1][2]
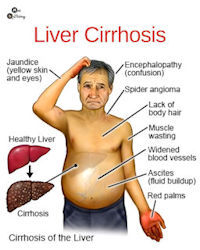
Major Complications of Cirrhosis
Decompensation arises from portal hypertension and hepatocellular failure. Ascites, the most common initial event, often requires diuretics and sodium restriction; refractory cases need repeated paracenteses. Esophageal/gastric varices pose catastrophic bleeding risk, managed with beta-blockers and endoscopic banding. Spontaneous bacterial peritonitis demands prompt antibiotics. Hepatic encephalopathy manifests as confusion or coma, treated with lactulose/rifaximin. Jaundice, coagulopathy, and hypoalbuminemia reflect synthetic dysfunction. Systemic consequences include sarcopenia despite fluid overload, hepatorenal syndrome (rapidly fatal without transplant), and heightened infection susceptibility. The first decompensating event signals a critical juncture—median survival drops sharply without transplantation, making early referral essential.[1][3]
Diagnosis, Staging, and HCC Surveillance
Diagnosis integrates clinical history, exam, labs, imaging, and sometimes biopsy. Noninvasive fibrosis assessment via transient elastography (FibroScan) or MR elastography is routine. Child–Pugh classifies functional reserve (A–C), while MELD-Na predicts 90-day mortality and drives allocation priority. Regular monitoring tracks rising MELD, refractory ascites, recurrent infections, or encephalopathy. Because cirrhosis confers the highest risk for hepatocellular carcinoma (HCC), guidelines mandate ultrasound ± AFP every 6 months—early detection dramatically improves curative options, including transplantation within Milan/UCSF criteria or down-staging protocols. Vigilant surveillance and timely intervention bridge patients safely toward transplant candidacy.[2][4]
When Liver Transplantation Becomes Necessary
Transplantation is the only curative therapy for decompensated cirrhosis and select HCC cases. Early referral—ideally at MELD-Na ≥15 or first major decompensation—allows comprehensive evaluation, comorbidity optimization, and education before irreversible decline. Common triggers include refractory ascites, recurrent variceal hemorrhage, hepatorenal syndrome, spontaneous bacterial peritonitis, or HCC meeting transplant criteria. Evaluation assesses extrahepatic organ function, nutrition, psychosocial support, and contraindications. Multidisciplinary input from surgeons, hepatologists, coordinators, social workers, and dietitians shapes individualized plans: active listing, bridging therapies, or palliative pathways. Transparent goals-of-care discussions empower informed decision-making and improve post-transplant outcomes.[3][5]

Optimizing Health While Awaiting Transplant
Excellent pre-transplant management stabilizes patients and improves post-transplant survival. Alcohol abstinence is non-negotiable. Sodium restriction (<2 g/day) and diuretics control ascites; high-protein nutrition (with encephalopathy-adjusted regimens) combats sarcopenia. Beta-blockers and endoscopic banding prevent variceal bleeding; lactulose/rifaximin manage encephalopathy. Vaccinations (hepatitis A/B, pneumococcal, influenza, COVID-19) are critical given infection vulnerability. Regular exercise, weight management in MASLD, and smoking cessation enhance resilience. Clear communication protocols, advance care planning, and caregiver involvement ensure rapid response to decompensation. Many patients live productively for years with compensated cirrhosis—diligent multidisciplinary care maximizes quality of life and transplant success when the time arrives.[1][4]
Medical Disclaimer
This information is for educational purposes only and is not a substitute for professional medical advice. Management of cirrhosis, timing of transplant referral, and candidacy decisions vary by center and patient. Always follow the individualized guidance of your hepatologist, transplant team, and healthcare providers.
References
- AASLD Practice Guidance on Risk Stratification and Management of Portal Hypertension and Varices in Cirrhosis (2024)
- EASL Clinical Practice Guidelines for the Management of Patients with Decompensated Cirrhosis (2018)
- When to Refer for Liver Transplantation: Expert Consensus (Transplantation 2025)
- Mayo Clinic – Cirrhosis: Diagnosis, Management, and Transplant Considerations
- Cleveland Clinic – Cirrhosis of the Liver: Complications and Transplant Evaluation